
Travel Health Tips
What do travel health clinicians tend to get wrong?

By Alys Bunce (RGN, PGCE)
Clinical Trainer in Phlebotomy, Travel Health and Immunisation.
One of the courses I teach most frequently is the travel health update course
Let's take a look shall we?
I absolutely adore meeting others with a similar passion to myself for this wonderful subject. A few hours just never feels enough for all the wonderful information that’s out there (to be fair though, a week still wouldn’t be enough), but I do my best to squeeze in as much as I can while still making it as engaging as possible.
One of the time-maximising techniques I use is my labour-of-love ‘travel vaccine quiz’. This is a self-directed quiz with loads of updates integrated into the automated feedback once it’s been submitted. Therefore, delegates can take the link away and complete it at their leisure after the course to squeeze in a few more of those all-important updates and find out what they need to read up on some more. It generally goes down very well and it is rare that a respondent gets above 50% so clearly it highlights lots of useful learning areas.
I want to share with you some of the results I’ve been accidently amassing*. It makes interesting reading and really helps me to plan for future courses. Mainly informed by which questions people tend to get wrong. So far, I’ve got over 200 participant answers to go on, which indirectly also gives us a good idea of common mistakes people make in practice.
*However, just to note - this is not like ‘proper research’, it’s just an informal quiz that happens to give me, and most importantly, delegates, an insight into where people need to brush up on.
A lot of people know very little about the vaccines they don’t provide.
It seems obvious that if you don’t give a vaccine, you are not likely to retain much information about its administration. People are busy, they have a lot to do, I totally get it. But the basics are really useful to know. For instance, 80% of my quiz respondents so far didn’t know that both tick borne encephalitis (TBE) and Japanese encephalitis (JE) vaccines have options for accelerated schedules. Could this be preventing them referring on if the traveller is a little short of time?
Key points to know about this:
- TBE: First two vaccines are generally 28 days apart but if time is short can be reduced to 14 days apart. Both schedules have a third dose at 5-12 months.
- JE: The two primary doses can be done in a week (0, 7) instead of a month (0, 28) in a certain age group.
- Of course, we must be mindful of the rule that you should always go for the longer option if you have time. But good to know for those last-minute travellers who ask ‘but do I have time for the course before I go?’. ‘Should I bother?’.
- Also, whichever vaccines you give or don’t give we all need to be discussing them all if we are performing a comprehensive travel health consultation. It’s not all about the vaccines - the advice is the bread and butter of travel health. Don’t shoot the messenger - it’s in all the guidance!
See here for the RCN Travel health competencies
See here for the RCPSG competencies
One does NOT need 17 hepatitis A boosters.
As you likely know already, the monovalent hepatitis A schedule is generally a dose on day 0 and another 6-12 months later for ideal continuous protection (which at-the-time-of-writing will then take you to at least 25 years before a booster is required).
A surprising amount of quiz respondents didn’t realise that you don’t have to start all over again if one turns up late for the 2nd dose. If a traveller turns up with a vaccine history of a first dose 5 years ago, then just give them the second and they will then have many more years (25 at least from that dose) of long-term protection. This applies to the majority of the vaccines, with some, but very few, exceptions. The immune system is crazy good. It will have a memory of that first priming dose and pick right up where it left off. Yes, for the last 4 years that traveller may have had a waning or even unacceptable hepatitis A titre, but the second dose is about CONTINUOUS protection and will bring immunity right back up again, even if it was delayed.
Incidentally although this rule applies to most vaccines there ARE some notable exceptions to not restarting if the primary schedule goes awry. Here are two such vaccines: Vivotif (oral typhoid) and Dukoral (oral Cholera).
I do wonder from the quiz answers how many people are walking around having been jabbed way too many times with hepatitis A? The NHS could be saving a fortune if everyone realised this! Don’t believe me? Take a look at the pie chart!
Want to see another pie chart? Here you go…. the red bits are the wrong answers.
Twinrix and monovalent hepatitis A: Never the twain shall meet.
The red section is the amount of people that have got the question wrong so far
A lot of quiz respondents have evidently been mixing Twinrix (hepatitis A and B combined) with monovalent hepatitis A, presumably blissfully unaware that there are differing hepatitis A contents in each. Stick to one or the other is mine and Green Book’s advice unless you really really don’t have any other option.
For example, those of you who have been doing it a while – remember those hepatitis A and B vaccine shortages several years ago where PHE (as they were known back then) temporarily said “anything goes – just get hepatitis A immunity in them in whatever way you can”? Well, we are well out of those shortages now. and we have to go back to being sensible again about juggling those Elisa units.
Not sure what I’m going on about? Try Jane Chiodini’s amazing free short course ‘hepatitis A Nuggets of Knowledge’ and it will all make sense. She’s the goddess of travel health and she will sort it all out for you in your mind if you’re a bit confused by the whole thing.
Or, of course, join a Dovetail update and I will explain it all properly to you and answer all your hepatitis A questions over a nice cup of tea and biscuits. (Face to face, we bring the biscuits, virtual courses require you to bring your own - but at least you get to choose your faves).
TB or not TB – that is the question. Nobody seems to know the answer though.
Again, a vaccine that a lot of people don’t give in a GP practice or a private travel clinic, therefore don’t know a lot about. Understandable again – you’re busy, you have enough to be getting on with. BUT did you know that BCG is the most WIDELY USEDVACCINE in the whole world? And active TB is HORRIBLE. It’s worth knowing a bit about.
However, it takes a whole day just to teach around this vaccine so even on a foundation travel health course it’s not feasible to put in so much about it. The highlights are thus:
- This is selectively advised. You won’t be recommending BCG vaccination much but when you do need to you REALLY need to. Don’t ignore the TB tab if it appears on your database for that country!
- Know your referral systems. Private travel clinics aren’t guaranteed to deliver it due to needing high demand for the multi-dose vial it’s supplied in (and short window from opening) so don’t assume everyone who’s private does it.
- Do a short course on TB to get a basic understanding of it.
- Know the interactions with other vaccines. See chapter 11 in the Green Book and read the Tuberculosis chapter too. Did you know that if someone has had a fresh BCG you can’t give another vaccine in the same arm for three months after? It is usually done in the left arm as specified by WHO.
- As I said, TB is horrible- and widespread. Although the vaccine isn’t the most effective, especially as one ages, always discuss the risks, signs and symptoms to travellers visiting high endemicity areas. Even if the vaccine itself isn’t indicated.
It’s not all work and no play. Business travellers have sex too!
Not always of course! But never underestimate the risk of hepatitis B and other STD’s in those rather safe-looking business trips. Did you know that it is custom in some countries to offer a ‘sex gift’ to high-flying businessmen and women? Perhaps a relaxing ‘massage’ with a ‘happy ending’? An attractive ‘concierge’ to escort them around town and ‘take good care’ of them? They have days off too. This can lead to anything… And there’s the more sombre risk, as there is with ANY traveller, of assault and rape abroad. Do not overlook the business traveller’s sexual health needs like people often do on my quiz.
Ticks Wanted! Dead or alive!

Do you know what to do with a tick you just pulled out of someone’s armpit or your dog? I ask this question on the update courses.
The answers are sometimes quite amusing -and brutal!! ‘Stamp on it’, ‘flush it’, take a flamethrower to it…’ and so on. Again, despite having been around a long time (many years) so many people still don’t realise there’s a UKHSA tick surveillance scheme going on.
The red bit in this pie chart indicates all the people
who evidently don’t know this.
Rather than explain it all here please visit the government resources page to find out more. One specific tip though (in case you don’t go there). Know that you can (and probably should) send your plucked out remains of ticks to the UKHSA for analysis - dead or alive! Basically, the UKHSA wants to examine ticks in the UK to find out what diseases they may be carrying and to look at the changing breeding patterns and species.
Could we have tick borne encephalitis (TBE) in the UK in our lifetime? Very likely, yes. Help the authorities to work out what’s going on. We have had cases of TBE transmitted in the UK and they are likely not the last. Could this vaccine be free on the NHS one day? Possibly. They are also looking at Lyme disease, also spread via the humble tick. And no, the TBE vaccines do nothing for preventing this one sadly. I get asked that one a lot.
Cholera vaccine is free! Catching it is too sadly.
Why do so many people not realise this vaccine is funded by the NHS? Probably because they are unaware of the reason why some vaccines are free and some are not. It's interesting to hear people’s attempts at guessing why some vaccines are free and some aren’t. And often one such guess often relates to how ‘common’ a disease seems to be. Cholera isn’t a frequently recommended vaccine therefore it's easy to see why people assume it may not be free.
However, here’s the rub: If you are capable of spreading the disease once you are back in the UK it’s likely going to be cheaper for the NHS to vaccinate one person than treat a whole load of people with that communicable disease who caught it from one traveller. Travel health vaccines given in the NHS are generally about protecting the UK from the traveller on their return. The UK is capable of experiencing hepatitis A, typhoid, diphtheria, polio and cholera outbreaks because of the way they are spread (faecal-oral route AKA ‘poo-in-the-mouth’). This is a large part why they are NHS funded and also an essential service.
Let’s take a look at a couple of the private vaccines to explore this more. Japanese encephalitis is spread by a mosquito that is not present in the UK. Yellow fever, again, spread by the pesky Aedes (mainly) which isn’t in the UK. Rabies - massively high risk in a lot of places in the world, but very low risk in the UK of human spread on return to the UK- unless there’s a zombie apocalypse and humans start biting humans after their travels (but then we have a whole lot more to worry about than rabies). Those diseases will generally only affect the traveller, not the rest of the UK.
Hence: privately funded.
BUT saying that- here’s one more commonly answered question that people get wrong.
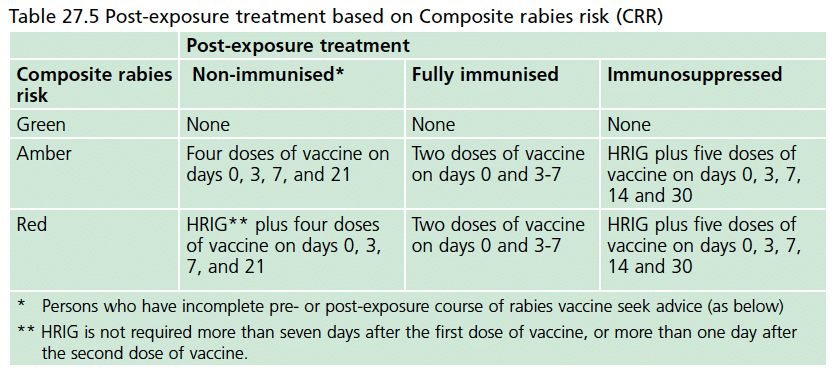
Rabies vaccine is always privately funded? … right? …
No. A very valuable NHS service is the post-exposure rabies consultation which absolutely can (and ideally should) be initiated through the NHS, pharmacies, and GP services. The schedule for post-exposure vaccines is easily sorted out through a phone call to the duty virologist at Colindale (or equivalent in Wales, Ireland and Scotland) - they even post the vaccines to the surgery the next day! Private clinics do it free too although they can charge consultation fees even though the vaccines themselves are free.
This is a horrible stealthy disease with an extremely high death rate for those who take their chances and wait for symptoms and therefore are too late for any treatment. All exposures in rabies endemic areas should be treated with the assumption it could mean rabies has been transmitted.
Have you thought about how you would handle it if during an interaction with a patient they announced they were bitten by a dog in Mexico 6 years ago and did nothing about it? There have been cases of rabies that have transpired up to 19 years (possibly more) after the exposure. Never too late to start the post-exposure vaccines! If this is a bit of a mystery to you then maybe it’s time for an update?
Ok, so I have concentrated on the wrong answers so far. What do the quiz respondents generally do well on?
- Knowing you’re able to give Typhim off label from 12 months and up if particularly high risk. It won’t work as well due to being a polysaccharide, of course, but it’s better than nothing. But you know this already.
- Knowing there is a live oral vaccine for typhoid. Good old Vivotif. But, have you used it yet in your clinic? Do you know how to if need arises? And why you might give Vivotif over Typhim? These are lesser known answers.
- Most quiz respondents are very good at advising not to drink tap water. In fact, there’s a 100% hit rate on that question. However, a lot of people don’t realise the huge variety of options about there for safe water, tending to stick with the advice of ‘drink bottled’.
I’m not against bottled water but would certainly advise to have a good look at the other options too. As a keen traveller myself here’s what I’ve witnessed with bottled water:
- Dogs urinating on crates stored ‘out the back’
- Rats running over crates (I.E. lids - the bit your mouth goes nearest to).
- Bottles being filled from taps and re-sealed with fancy equipment then sold again
- Shops being few and far between and even more variation in opening times
- Lots and lots of plastic pollution
Do try to encourage your travellers to consider other more sustainable, cheaper and possibly even safer options. All of which we can discuss on a course together if you are not too sure what they are.
Anyway, that’s all just the tip of the iceberg.
There's loads more I want to tell you!!! And I want to hear all YOUR questions and help you to figure out the answers. Sign up for a Dovetail course and I’ll give you all the tips and refreshers you need for performing your best ever travel health consultations. Maybe you will be kind enough to share some of your tips with me too? We ALL clearly have a lot to learn in this massive, and amazing, subject area!!
